www.theoxfordscientist.com
Joe Biden - Kamala Harris
President & Vice President
of the United State of America
President & Vice President
of the United State of America

|
|

|
... America, can breathe, again
I trust the introductory email to this communication was met with sufficient interest to occasion your personal perusal of this material.
... a mask in time, saves nine
The importance of wearing a mask from a clinical perspective, equates the severity of coronavirus symptoms to the number of viral particles inhaled, and whether the infection was the result of a singular or multiple exposures.
After a deluge of requests, to state whether the preceding statement was accurate or otherwise, the CDC-USA, in a written statement issued on the 22 of October 2020, not surprisingly, confirmed its accuracy, while at the same time substituting the word cumulative for this author's suggested terminology, multiple exposures. We will return to the importance of terminology in the section on waves vis-à-vis spikes and surges.
There are four principal criteria to be applied to the evaluation of the efficacy and effectiveness of a face mask, especially a mask to be used to contain the spread of the SARS-CoV-2 virus i.e., breathability, fit, pore size and whether the material from which the mask is made is hydrophobic (moisture repellent), or hydrophilic (moisture attracting).
After stating the obvious, one is confronted often with the phrase that 'it goes without saying' or other words which convey the same meaning, as is the case with our first criteria of evaluation. The first criteria concerns, breathability, that is, the wearer of the mask must be able to breathe properly through the mask. Otherwise, its use would be counterproductive, in the extreme.
The second criteria, fit, encompasses both the ability of the mask to cover both the nose and mouth, while at the same time, the mask must prevent the aerosol containing the airborne viral particles from entering the nose and mouth area through the fabric of the mask, as well as, from around the perimeter of the mask. In this specific regard, fit, the respirator might prove the preferred face-mask device.
Pore size, the third principal criteria, takes into consideration the size of the virus-laden aerosol particles, otherwise known as droplets and spray, from passing through the fabric of the mask.
A N95 grade mask, for example, is rated by different observers as having the ability to screen between 85 to 95% of air-borne particles smaller than 300 nanometres. The nanometre is a unit of length in the metric system, equal to one billionth of a metre, and is expressed in scientific notation as 1×10⁻⁹ metre.
At the same time, as we have suggested above, the wearer must be able to breathe normally, that is, without restricting the wearer's ability to take in a sufficient amount of air to sustain life.
The size of the aerosol, droplets and spray, emitted into the air by a coronavirus disease carrier through coughs, sneezes, talking and breathing, varies between 65 to 125 nm. Therefore, a mask must be able to prevent particles of this size from flowing through it to be an effective barrier.
The aerosol, droplets and spray, that a carrier emits into the air is moist, which necessitates that the material from which the mask is made should be hydrophobic, moisture repelling.
If, the material is hydrophilic, moisture attracting, the pores of the mask material will trap virus laden particles, and make it possible for the wearer to draw virus through the mask as the pores become increasingly saturated, clogged, with moist virus-laden particles.
There are mask-like products on the market which suggest that they can also be used as cooling devices by soaking them in water prior to use.
At the same time, recent advances in mask technology should be incorporated into future containment strategies (1).
There simply are no national evidence-based standards for face masks. And yet, the face mask remains a heralded pre-vaccine containment measure along with social distancing, the ubiquitous quarantine, and sheltering-in-place.
1. A Flexible Nanoporous Template for the Design and Development of Reusable Anti-COVID-19 Hydrophobic Face Masks. ACS Nano. 20 May 2020. DOI: 10.1021/acsnano.0c03976
Best regards,
E LaMont Gregory MSc (Oxford)
E LaMont Gregory MSc (Oxford)
___ ___ ___
... Humpty Trumpty never built the wall,
And yet, Humpty Trumpty still had a great fall,
And all the would-be-king’s nationalistic force,
Proved no match for democratic recourse.
And so the saga of Donald J Trump will be told,
In the annals of the country he so cheaply sold,
And they follow him blindly, shouting, 'lock her up',
While this great country they so shamelessly disrupt.
In a din, they chanted, make America great again,
In reality, America was never actually on the mend,
An election returned America to a sense of sober glee,
And with his passport secured, he cannot flee.
... Humpty Trumpty never built the wall,
And yet, Humpty Trumpty still had a great fall,
And all the would-be-king’s nationalistic force,
Proved no match for democratic recourse.
And so the saga of Donald J Trump will be told,
In the annals of the country he so cheaply sold,
And they follow him blindly, shouting, 'lock her up',
While this great country they so shamelessly disrupt.
In a din, they chanted, make America great again,
In reality, America was never actually on the mend,
An election returned America to a sense of sober glee,
And with his passport secured, he cannot flee.
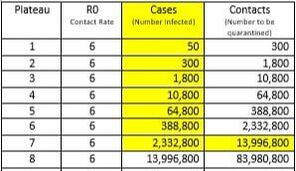
The table above should be understood as follows. Consider the 50 cases of infection identified at the Plateau 1 level. It has been established that each infected person can infect, on average, six (6+) other persons i.e., R0 (R-zero factor of 6+).
The R-zero factor of six (6) was obtained from calculations made in the early days of the novel coronavirus outbreak, when researchers around the globe still had access to data from several southeast Asian countrie, including welth of Dt from Hubei
And, this is the crux of the matter. Once you have 50 infections, and you do not want to progress to Plateau 2, 300 cases, you must track the initial 300 contacts from Plateau 1, and quarantine them immediately subject to testing, that is, contact justifies being placed in quarantine, and testing alone can release one from being quarantined.
One individual in New Rochelle, New York, confirmed to have been infected with the novel coronavirus, had close contact with 50 other persons through his business and through attendance at religious services. Each of his contacts had close contact with, on average, 6 other persons, 6 x 50 = 300. Each of these contacts, in turn, had contact with 6 others, and by this juncture, therefore, there were some, 6 x 300 = 1800, persons possibly infected with the virus in that area.
Governor Andrew Cuomo of New York then ordered National Guard troops into New Rochelle. And, as discussed in the previous communication - https://www.theoxfordscientist.com/coronavirus-the-second-wave.html - this move was welcomed literally around the globe. From Milan, where health workers found it difficult to awaken Italian authorities to the true nature and scope of the coronavirus outbreak, to Iceland where an American company operating in Iceland helped the identification and tracing of some 7800 people who had had contact with the first 600 cases on that island, by providing the test kits for the coronavirus.
The sense of anticipation associated with the Cuomo troop call up for those in Milan, who desperately wished to implement an identification and tracing program, and those in Reykjavik, Seoul, Shanghai and Taipei who implemented identification and tracing programs, although not emanating from Washington, was that the Americans were going to be the example of how a program of identification and tracing could be implemented in a liberal democracy, and take the US off the unrestrained exponential coronavirus growth curve.
But inexplicably, rather than deploy the troops to the task of augmenting the ability of the local health departments to carry out a rigorous tracing program to locate all those who may have been infected, as successfully demonstrated in Iceland and elsewhere, the troops became glorified traffic watchers and played no active part in the infectious disease control process.
The sense of anticipation turned to palpable dismay.
At 11am EST, on the morning of the 27th of April 2020, the Canada.ca website records 14,856 persons infected with the coronavirus in Ontario. That number, if the present means of infectious disease mitigation, which relies primarily on hygiene and social distancing, remains the primary means of infectious disease control, that number having surpassed the 10,800 plateau, will rise to the next plateau of 64,800 persons infected with coronavirus in Ontario.
Just as, once the total number of cases in the United States exceeded 388,800, it became inevitable that that number would rise to 2,332,800. It should be noted that in the last 30 days, total US cases have risen from approximately 388,800 to over one million cases of infection with the coronavirus.
In Alberta, where the number of known infections on the 28th of April stood at 4,850, again, it is inevitable, barring the immediate implementation of a case identification and contact tracing effort involving some 29,100 contacts with those known to be infected, Alberta will reach the next plateau of 10,800 infections in the near future.
Having witnessed hundreds upon hundreds die in long-term care facilities, when a stringent protocol of case identification and screening for all patients and all caregivers was suggested and ignored by both our professional health authorities and political leaders, but remains the most prudent means to curtail the spread of coronavirus in long-term care facilities, it is difficult to understand what will trigger the rigorous implementation of screening for the coronavirus to protect those in long-term care.
The R-zero factor of six (6) was obtained from calculations made in the early days of the novel coronavirus outbreak, when researchers around the globe still had access to data from several southeast Asian countrie, including welth of Dt from Hubei
And, this is the crux of the matter. Once you have 50 infections, and you do not want to progress to Plateau 2, 300 cases, you must track the initial 300 contacts from Plateau 1, and quarantine them immediately subject to testing, that is, contact justifies being placed in quarantine, and testing alone can release one from being quarantined.
One individual in New Rochelle, New York, confirmed to have been infected with the novel coronavirus, had close contact with 50 other persons through his business and through attendance at religious services. Each of his contacts had close contact with, on average, 6 other persons, 6 x 50 = 300. Each of these contacts, in turn, had contact with 6 others, and by this juncture, therefore, there were some, 6 x 300 = 1800, persons possibly infected with the virus in that area.
Governor Andrew Cuomo of New York then ordered National Guard troops into New Rochelle. And, as discussed in the previous communication - https://www.theoxfordscientist.com/coronavirus-the-second-wave.html - this move was welcomed literally around the globe. From Milan, where health workers found it difficult to awaken Italian authorities to the true nature and scope of the coronavirus outbreak, to Iceland where an American company operating in Iceland helped the identification and tracing of some 7800 people who had had contact with the first 600 cases on that island, by providing the test kits for the coronavirus.
The sense of anticipation associated with the Cuomo troop call up for those in Milan, who desperately wished to implement an identification and tracing program, and those in Reykjavik, Seoul, Shanghai and Taipei who implemented identification and tracing programs, although not emanating from Washington, was that the Americans were going to be the example of how a program of identification and tracing could be implemented in a liberal democracy, and take the US off the unrestrained exponential coronavirus growth curve.
But inexplicably, rather than deploy the troops to the task of augmenting the ability of the local health departments to carry out a rigorous tracing program to locate all those who may have been infected, as successfully demonstrated in Iceland and elsewhere, the troops became glorified traffic watchers and played no active part in the infectious disease control process.
The sense of anticipation turned to palpable dismay.
At 11am EST, on the morning of the 27th of April 2020, the Canada.ca website records 14,856 persons infected with the coronavirus in Ontario. That number, if the present means of infectious disease mitigation, which relies primarily on hygiene and social distancing, remains the primary means of infectious disease control, that number having surpassed the 10,800 plateau, will rise to the next plateau of 64,800 persons infected with coronavirus in Ontario.
Just as, once the total number of cases in the United States exceeded 388,800, it became inevitable that that number would rise to 2,332,800. It should be noted that in the last 30 days, total US cases have risen from approximately 388,800 to over one million cases of infection with the coronavirus.
In Alberta, where the number of known infections on the 28th of April stood at 4,850, again, it is inevitable, barring the immediate implementation of a case identification and contact tracing effort involving some 29,100 contacts with those known to be infected, Alberta will reach the next plateau of 10,800 infections in the near future.
Having witnessed hundreds upon hundreds die in long-term care facilities, when a stringent protocol of case identification and screening for all patients and all caregivers was suggested and ignored by both our professional health authorities and political leaders, but remains the most prudent means to curtail the spread of coronavirus in long-term care facilities, it is difficult to understand what will trigger the rigorous implementation of screening for the coronavirus to protect those in long-term care.

