www.theoxfordscientist.com
Transmission date: 12 May 2020 - Publication date: 12 May 2020 - distribution list includes Governor DeWine of Ohio, Mayor Lightfoot of Chicago
... a perfect storm
A perfect storm, is an idiom, formulaic language as it were, used to describe
a rare combination of events creating an unusually bad situation, and is
an apt descriptor for the havoc wrought by the novel coronavirus pandemic.
... social distancing and hygiene, are protective measures designed to increase the effectiveness
of the two most essential means of infectious disease control, case identification & contact tracing.
... social distancing and hygiene cannot replace, case identification & contact tracing,
as the most effective means of infectious disease control.
Stated in terms that are unequivocal:
It must be understood that there is no discernible pathway to control the spread and
devastating onslaught of the coronavirus pandemic, before the availability of an efficacious vaccine,
which does not have at its core, a rigorous program of case identification and contact tracing.
For the most part, our present circumstances exist,
because no such undertaking has, to date, been forthcoming.
E LaMont Gregory MSc Oxon
Since my last communication, which contained a protocol, a by-the-book, evidence-based approach to protecting those in long-term care from exposure to the coronavirus, and that advice seems to have been ignored largely, and with horrific results.
Observing that all knowledge is comparative, the contrast in outcomes between the nursing homes and long-term care facilities in the community of Villanova, on the outskirts of Lyon, France, and those same facilities in Ontario could not be more instructive as to how one goes about protecting vulnerable populations.
Having committed to engage 'every single measure possible', the Ontario Minister of Long-term Care will surely acquaint herself with the facts of Villanova, as should the many others who share her awesome responsibilities.
There should be no doubt that a 15-minute coronavirus test, which ushers in the ability to know whether a person is positive for the novel coronavirus in real time, instituted properly, will prove beneficial.
Importantly, the 15-minute coronavirus test, when implemented properly, can help reduce the iatrogenic transmission of the coronavirus by health care workers, caregivers, as well as essential services personnel, to a minimum.
As an example, let us consider shift change at a fire or a police station. All personnel entering the station report 20 minutes to 1/2 hour, on the clock as it were, before the start of their duty. They drive through the mobile testing station, get swabbed, proceed to the parking lot, and are notified of the result of their test within 1/2 hour. If, the test is negative, they proceed into the station.
Those leaving the station go through the same procedure. All personnel whose duty requires them to remain in the station, depart with those leaving the station and proceed to the testing area for those seeking to enter, and are tested before they re-enter the station.
In a previous communication, this author, based on the lesson of the second wave of SARS 2002-2004, suggested that all patients in hospital with pneumonia be tested for the coronavirus. This becomes possible in real time with the 15-minute coronavirus test.
As in the case of firefighters and police, all healthcare workers, in fact, everyone entering a hospital or any care facility, is screened before they enter. If, they test negative, they proceed to their stations or work areas. It is this group of health workers that screens all the patients in hospital. All workers leaving are tested and if any tests positive, and if they are qualified to do so, before they leave the parking lot, they are supplied with enough kits to test all those in their own household, or anyone else they have come into contact with within their own home, in which they will now be self quarantined.
The same testing regime, as a matter of the utmost urgency, must be implemented in all nursing homes, long-term care facilities, hospice care centers and Veterans' hospitals. Everyone must be screened entering, and those cleared to enter test all residents in the facility. Again, all workers remaining at shift change, depart the facility with other workers ending their shift and join the queue of those being tested to enter the facility, without exception.
Evidence supports the realization that those in hospital being treated for pneumonia, those in-hospital patients with immunodeficiency disorders, the elderly in nursing homes, our veterans in VA hospitals, and all those under hospice care, and those that care for them, must be tested for the coronavirus. And, the 15-minute coronavirus test, implemented properly, is a reasonable means to achieve this objective.
To have the 15-minute test and not implement a procedure to protect the public generally, as well as our most vulnerable and essential workers, ought to be unthinkable.
Reykjavik, Seoul, Shanghai and Taipei
|
|
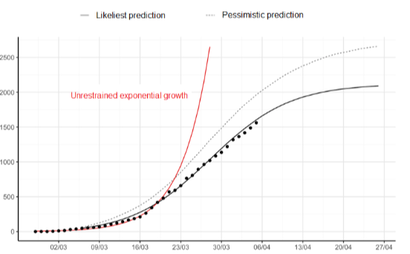
The graph on the left illustrates the course of coronavirus infections in Iceland from the 2nd of March to the 6th of April,
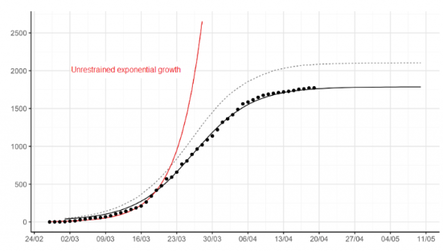
the graph on the right bring that information forward to include infections recorded through the 20th of April.
Click on the link, below, to read the full report of the Covid-19 mitigation campaign in Iceland, conducted by the
Health Sciences Institute of the University of Iceland, the Directorate of Health, and the National Hospital of Iceland -
https://covid.hi.is/english/
the graph on the right bring that information forward to include infections recorded through the 20th of April.
Click on the link, below, to read the full report of the Covid-19 mitigation campaign in Iceland, conducted by the
Health Sciences Institute of the University of Iceland, the Directorate of Health, and the National Hospital of Iceland -
https://covid.hi.is/english/
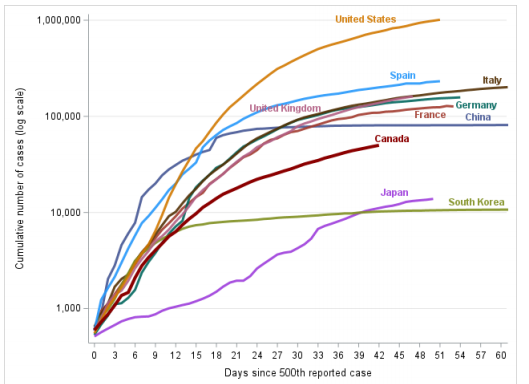
The red line, above, illustrating 'Unrestrained exponential growth' of the spread
of the coronavirus, is exactly what is occuring in Canada and the United States.
Kindly, pay particular attention to the point in the above chart, when the solid line
with the superimposed dots, moves to the right of the red line representing unrestrained
exponential growth of coronavirus infections, which took place just before the 23rd of March.
This is a direct result of the case identification and contact tracing initiative conducted by
Icelandic health department's infectious disease control program.
All the resources necessary to identify and trace the contacts of those known to be infected in
New Rochelle and to quarantine all those who had close contact with those infected was in place.
The failure to do so, begs the question what have the 2800 and the 126 heads of our health
departments and health regions in the United States and Canada, respectively, been doing
since the coronavirus outbreak began in their respective districts and regions.
It will not go unnoticed that the vast majority of those who head the 2926 health
departments across Canada and the United States are political appointees.
The lesson here is that the results achieved by the health officials in Reykjavik, Taipei, Seoul and Shanghai,
could have been achieved in Milan, London, New York, Chicago, Seattle and Toronto, if the health officials
in those cities had implemented the most rudimentary infectious disease control strategies from the
onset of the outbreak of the coronavirus in their cities i.e., case identification and contact tracing.
of the coronavirus, is exactly what is occuring in Canada and the United States.
Kindly, pay particular attention to the point in the above chart, when the solid line
with the superimposed dots, moves to the right of the red line representing unrestrained
exponential growth of coronavirus infections, which took place just before the 23rd of March.
This is a direct result of the case identification and contact tracing initiative conducted by
Icelandic health department's infectious disease control program.
All the resources necessary to identify and trace the contacts of those known to be infected in
New Rochelle and to quarantine all those who had close contact with those infected was in place.
The failure to do so, begs the question what have the 2800 and the 126 heads of our health
departments and health regions in the United States and Canada, respectively, been doing
since the coronavirus outbreak began in their respective districts and regions.
It will not go unnoticed that the vast majority of those who head the 2926 health
departments across Canada and the United States are political appointees.
The lesson here is that the results achieved by the health officials in Reykjavik, Taipei, Seoul and Shanghai,
could have been achieved in Milan, London, New York, Chicago, Seattle and Toronto, if the health officials
in those cities had implemented the most rudimentary infectious disease control strategies from the
onset of the outbreak of the coronavirus in their cities i.e., case identification and contact tracing.
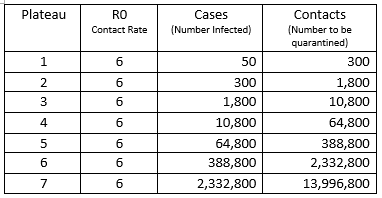
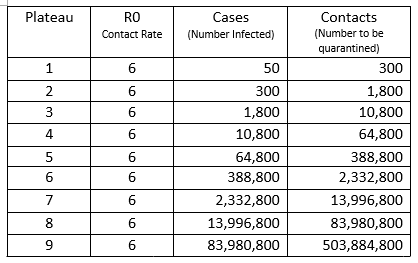
The table above should be understood as follows. Consider the 50 cases of infection identified at the Plateau 1 level. It has been established that each infected person can infect, on average, six (6+) other persons i.e., R0 (R-zero factor of 6+).
And, this is the crux of the matter. Once you have 50 infections, and you do not want to progress to Plateau 2, 300 cases, you must track the initial 300 contacts from Plateau 1, and quarantine them immediately subject to testing, that is, contact justifies being placed in quarantine, and testing alone can release one from being quarantined.
One individual in New Rochelle, New York, confirmed to have been infected with the novel coronavirus, had close contact with 50 other persons through his business and through attendance at religious services. Each of his contacts had close contact with, on average, 6 other persons, 6 x 50 = 300. Each of these contacts, in turn, had contact with 6 others, and by this juncture, therefore, there were some, 6 x 300 = 1800, persons possibly infected with the virus in that area.
Governor Andrew Cuomo of New York then ordered National Guard troops into New Rochelle. And, as discussed in the previous communication - https://www.theoxfordscientist.com/coronavirus-the-second-wave.html - this move was welcomed literally around the globe. From Milan, where health workers found it difficult to awaken Italian authorities to the true nature and scope of the coronavirus outbreak, to Iceland where an American company operating in Iceland helped the identification and tracing of some 7800 people who had had contact with the first 600 cases on that island, by providing the test kits for the coronavirus.
The sense of anticipation associated with the Cuomo troop call up for those in Milan, who desperately wished to implement an identification and tracing program, and those in Reykjavik, Seoul, Shanghai and Taipei who implemented identification and tracing programs, although not emanating from Washington, was that the Americans were going to be the example of how a program of identification and tracing could be implemented in a liberal democracy, and take the US off the unrestrained exponential coronavirus growth curve.
But inexplicably, rather than deploy the troops to the task of augmenting the ability of the local health departments to carry out a rigorous tracing program to locate all those who may have been infected, as successfully demonstrated in Iceland and elsewhere, the troops became glorified traffic watchers and played no active part in the infectious disease control process.
The sense of anticipation turned to palpable dismay.
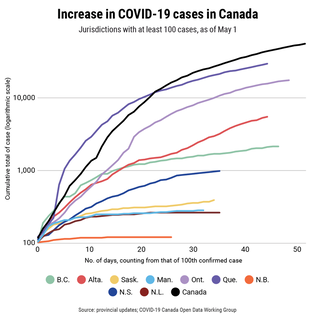
At 11am EST, on the morning of the 27th of April 2020, the Canada.ca website records 14,856 persons infected with the coronavirus in Ontario. That number, if the present means of infectious disease mitigation, which relies primarily on hygiene and social distancing, remains the primary means of infectious disease control, that number having surpassed the 10,800 plateau, will rise to the next plateau of 64,800 persons infected with coronavirus in Ontario.
Just as, once the total number of cases in the United States exceeded 388,800, it became inevitable that that number would rise to 2,332,800. It should be noted that in the last 30 days, total US cases have risen from approximately 388,800 to over one million cases of infection with the coronavirus.
In Alberta, where the number of known infections on the 28th of April stood at 4,850, again, it is inevitable, barring the immediate implementation of a case identification and contact tracing effort involving some 29,100 contacts with those known to be infected, Alberta will reach the next plateau of 10,800 infections in the near future.
Having witnessed hundreds upon hundreds die in long-term care facilities, when a stringent protocol of case identification and screening for all patients and all caregivers was suggested and ignored by both our professional health authorities and political leaders, but remains the most prudent means to curtail the spread of coronavirus in long-term care facilities, it is difficult to understand what will trigger the rigorous implementation of screening for the coronavirus to protect those in long-term care.
Medical Practice in the Time of the Coronavirus Pandemic
This author is aware fully, of the competing demands on medical services wrought on by the coronavirus pandemic.
I had a professor in a subject that concerns matters of national security i.e., pro aris et focis, who had been a successful field commander in the European theatre during WWII. He was called back to Washington by FDR to be his liaison between the White House and the Department of War.
Many commanders noticed that some of the best commanders were being reassigned at a time when they were engaged in major battles, and naturally they complained to FDR. And, were often dismayed to receive a response which basically instructed them to continue to engage the enemy, even if their resources were only frightfully marginally superior to those of the opposing forces, and to do so in a way that would inflict maximum damage to the opposing forces, while causing minimal casualties within their own troops.
What the field commanders did not know, was that plans were underway for D-Day, because if there was going to be a D-Day, it had to be planned for, and planning requires the use of resources, or there was not going to be a D-Day. And, a significant part of that plan called upon them to continue to engage the enemy, as best they could.
So, naturally, this author understands that while the prime minister and the premiers to whom this communication is addressed, Justin Trudeau, Jason Kenney and Doug Ford, are rightfully engaged in the war against the coronavirus, there are other battlefields which require their earnest attention, as well.
With that introduction, I draw your attention to our Ophthalmologists during the pandemic, those whose remit is to preserve sight, correct visual impairments and to prevent blindness.
Surely, there can be no notion that there is even a hint of a tradeoff between preventing the spread of the coronavirus and the loss of one's ability to see? And yet, the quality of life and the eyesight of hundreds of cataract and glaucoma patients in need of eye surgeries deteriorate every week in Edmonton alone due to the near cessation of eye surgeries.
The issue for the consideration of our political leaders, seeking as they do, the advice of their appointed heads of our health services, is to avoid the belief that the backlog problem might be cured by a return to a spattering of eye surgery services about the city.
When in reality, the realization of the Eye Hospital, the result of decades of effort to centralize eye care into a center of excellence, where research and training have brought about advances in eye care unimaginable in a decentralized system. Therefore, experience has taught us that the solution to the backlog problem does not lie in the recreation of decentralized eye surgery services.
I had a professor in a subject that concerns matters of national security i.e., pro aris et focis, who had been a successful field commander in the European theatre during WWII. He was called back to Washington by FDR to be his liaison between the White House and the Department of War.
Many commanders noticed that some of the best commanders were being reassigned at a time when they were engaged in major battles, and naturally they complained to FDR. And, were often dismayed to receive a response which basically instructed them to continue to engage the enemy, even if their resources were only frightfully marginally superior to those of the opposing forces, and to do so in a way that would inflict maximum damage to the opposing forces, while causing minimal casualties within their own troops.
What the field commanders did not know, was that plans were underway for D-Day, because if there was going to be a D-Day, it had to be planned for, and planning requires the use of resources, or there was not going to be a D-Day. And, a significant part of that plan called upon them to continue to engage the enemy, as best they could.
So, naturally, this author understands that while the prime minister and the premiers to whom this communication is addressed, Justin Trudeau, Jason Kenney and Doug Ford, are rightfully engaged in the war against the coronavirus, there are other battlefields which require their earnest attention, as well.
With that introduction, I draw your attention to our Ophthalmologists during the pandemic, those whose remit is to preserve sight, correct visual impairments and to prevent blindness.
Surely, there can be no notion that there is even a hint of a tradeoff between preventing the spread of the coronavirus and the loss of one's ability to see? And yet, the quality of life and the eyesight of hundreds of cataract and glaucoma patients in need of eye surgeries deteriorate every week in Edmonton alone due to the near cessation of eye surgeries.
The issue for the consideration of our political leaders, seeking as they do, the advice of their appointed heads of our health services, is to avoid the belief that the backlog problem might be cured by a return to a spattering of eye surgery services about the city.
When in reality, the realization of the Eye Hospital, the result of decades of effort to centralize eye care into a center of excellence, where research and training have brought about advances in eye care unimaginable in a decentralized system. Therefore, experience has taught us that the solution to the backlog problem does not lie in the recreation of decentralized eye surgery services.
Ventilators and respiratory therapy
From time to time there are events covered on cable news networks that stand as stark reminders that the news presenters are for the most part actors, and that cable news like all of the licensed channels on television, serve two cardinal functions for which television is well suited, that is, to inform and to entertain. And, there is often no clear demarcation between their informational and their entertainment programming.
Cable news networks are, in fact and in law, businesses supported by corporate advertisers. The advertising, and therefore corporate advertisers, pay for the operation of the news broadcasts and the salaries of the actors to draw audiences, from which a number of viewers will be influenced to buy or to subscribe to the products or services of the corporate advertisers, or they would not pay to advertise on them.
In part, this explains the almost universal pro-business bias of the cable news and entertainment outlets. Stephanie Ruhle, among many others, is a sterling example of this fact.
And, with this understanding of the cable news business, the constant spouting of the mantra that suggests that we just got to get the economy going, relax protective measures, which are designed to augment the most effective means of infectious disease control i.e., case identification and contact tracking, which to date are still in the rudimentary stages of implementation, and in very few places, makes sense.
Recently, one of the cable news networks covered the story of what they described as the suicide of a New York City hospital emergency room doctor, who according to the cable network 'was distraught over the coronavirus pandemic'.
The first news cycle of this story presented the doctor sympathetically and spoke of the shock and horror of the loss of a dedicated doctor.
The second news cycle brought a grieving close relative to the screen in a segment that was, in a word, heart wrenching. By the third and final cycle of the story the issue was framed as one of mental health and the station launched a crusade-like campaign for mental health assistance for all healthcare workers, who witness day after day the horrific loss of life that is the success story trumpeted by the president's son-in-law.
This same network, less than a fortnight later, before airing the bloodcurdling video of the savage slaying of an unarmed man in Georgia, stated that there had been crime in the area, and the three men, two armed and another prepared to film the encounter were looking for the perpetrator. And, the slain man just happen to have fit the profile.
This news item had been cleared by the forward planning department of the station, scripted, and this is the story they used to introduce the horrific video. Where did this story come from? There is no evidence that there is one scintilla of truth in it. This story could only have come from the local police department itself, whose relationship to the killers is the subject of a major investigation. But this is the story broadcast in association with airing the murderous video.
The emergency room doctor, as described on cable news, was in fact, the Medical Director of the Emergency Department of a Manhattan-based tertiary-care teaching hospital renown for excellence in clinical care. And, consider that the three cycle yarn created in the cable news studio, like their coverage of the Georgia extra-judicial murder mirrors the public relations strategy of 'getting out in front of the story'. And, the criminal justice establishment in Glynn County, Georgia, and the directors and administrators of New York City hospitals, and the mayor of New York City and New York governor Cuomo, all seem duly satisfied with their reporting.
Both cable news reports lack a modicum of anything resembling investigative reporting. We see a grieving relative mourning their loss, but no investigation of the actual working conditions in the hospitals, and no hint of probing interviews with her staff or colleagues. or even the medical directors of the emergency department of other hospitals. In the reporting of the Georgia jogger murder, cable news spun the normal feeding frenzy associated with the shooting of unarmed minorities.
Whenever one attempts to unravel a medical mystery, which the demise of a emergency room director during a pandemic is, surely. One begins by gaining an understanding of what is considered to be normal practice. First, within the hospital generally, and then the practice guidelines for each department, and finally the standard procedure manual for each individual ward, within each department.
Ventilators, mechanical respiratory assistance devices, have been a feature of the medical equipment necessary to treat those seriously or critically ill, due to their exposure and sebsequent infection with the novel coronavirus. A virus that attacks lung tissue in such a way as to impair the bodies ability to provide sufficient oxygen to maintain homeostatis, and thereby, to sustain viability.
... an utter lack of professional and public accountability
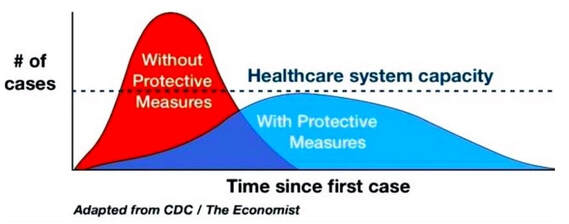
The graph above was one of the first to be released by the Center for Disease Control (CDC) at the same time the Trump Administration positioned VP Mike Pence to control the flow of information from the administration on all matters concerning the coronavirus pandemic. The Economist then adapted it, and spread it around the English-speaking world.
This graph provides a direct insight into what the administration in Washington believed and what the administration understood about the coronavirus, the nature and scope of its spread, as well as, whether mitigation efforts were called for or even necessary to counter the relentless advance of the novel coronavirus.
The graph depicts two patterns of virus spread. The red pattern describes the spread of the disease, without protective measures being implemented, while the area in blue illustrates the course of the disease spread with the implementation of protective measures.
The protective measures envisioned by the Trump administration, it must be understood, were limited to social distancing and hygiene measures, but there is no indication or written evidence that the two most important means of infectious disease containment, i.e., case identification and contact tracing ever entered the lexicon or thinking of Trump administration officials.
Further, the vertical axis indicates the number of people infected, # of cases. While the horizontal axis represents the passage of time, beginning with the first case of infection, and ostensibly, since both curves end when they return to the timeline, reasonable interpretation is that that is representative of the last case of infection.
Midway on the vertical axis, # of cases, there is a serrated line running parallel to the timeline, illustrating that as the number of cases increases, a point is reached, when the ability to care for any additional cases exceeds healthcare system capacity, that is, there are more people seeking assistance than there are healthcare workers and medical equipment to provide that assistance. Thus, at that juncture the healthcare system capacity has been exceeded.
Once health system capacity is exceeded, it is reasonable to surmise that the infected individuals represented by the area under the red curve above the serrated line would have no organized professional healthcare assistance available to them. Without such assistance, they would be condemned.
It should be remembered that the area in red above the serrated line occupies 45% of the total area of the red curve.
Let us turn our attention to the area under the red curve as opposed to the area under the blue curve. There are several ways of determining the area within the red and blue curves, it can be calculated mathematically, there are computer programs that would allow you to trace the circumference of the red and blue area and it will automatically calculate the area for you.
However, it is possible to simply grid the entire graph and count the squares in the red area, and in the blue area, and by doing so we quickly discover that the area in red and the area in blue occupy the same amount of space in this graph. The implications of that fact are far reaching and worthy of our utmost attention.
This graph illustrates what Trump often expressed in words, that is, that implementing a system with protective measures and not implementing a system with protective measures would result in the same number of cases.
Remembering, that above the red curve includes a period of time when the number of cases exceeds healthcare system capacity, and that the area in red above the serrated line occupies 45% of the total area of the red curve.
It should also be noted that the red area is above the serrated line for nearly one half of the amount of time from when the red curve rises above the timeline, until the red curve returns to the timeline.
And, as depicted, the red curve (doing nothing as far as protective measures are concerned), returns to the timeline in one half of the time that it takes for the blue curve (indicating the implementation of protective measures), to return to the timeline.
The message the Trump Administration and the CDC sought to convey to the American people was that doing nothing would end the coronavirus pandemic in one half the time it would take if protective measures were taken.
This is blatantly false!
It should also be understood that the current administration wanted the public to believe that although there would be a period of time when healthcare system capacity would be exceeded inflicting horrific numbers of premature deaths, nonetheless doing nothing would not cause any additional cases of infection with the virus, as illustrated by the area under the red and blue curves being the same.
The most generous interpretation of this graph is that it is an example of the utter lack of professional and public accountability, on the part of the CDC and the Trump administration.
And, this graph may also explain, why the 2800 health department heads across the United States, each and every one of whom understood that case identification and contact tracing stands as the most important means, pre-vaccination, for the control and containment of any infectious disease, did nothing, but let the novel coronavirus take hold.
|
|
text in process


To keep up with the articles on this site, join World Wide Auto Surf, by clicking on the image, above.
