www.theoxfordscientist.com
updated -- 7 May 2020 - Oxford Textbook of Infectious Disease Control - Cuomo & New Rochelle - Iceland - St Albert: 4, 20+, 100+ - Lightfoot & Chicago
Coronavirus Pandemic, the second wave
preparedness and response
preparedness and response
... the crisis in the greater New York City area vis-à-vis the coronavirus
pandemic, exists because, the initial response by the infectious disease
control management bureaucracy was conducted with Neolithic incompetence.
... wrought on by an utter absence, in the all important initial phase, of a
properly implemented infectious disease control surveillance strategy and
a rigorous contact management action plan.
... there is still time for Chicago and St Albert to get it right, in both instances,
however, it will require a Herculean effort, but only a Herculean effort.
E LaMont Gregory MSc Oxon
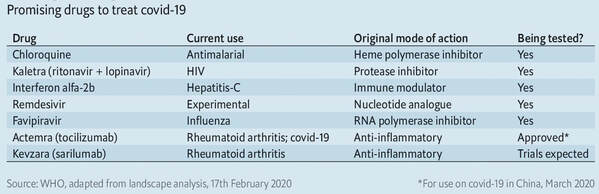
List of drugs suggested to be of potential therapeutic benefit in the treatment of CoV-19
In scientific terms, we are in the first wave of a 100-year pandemic event, a second, and perhaps, a third wave will follow. Those eventualities, however, are very much dependent on how well we conduct our current campaign against the first wave.
... the 15-minute coronavirus test, when implemented properly,
will reduce the iatrogenic transmission of the coronavirus by health care workers,
caregivers & essential services workers, and all with whom they interact to a minimum.
... it should not go unnoticed, how quickly the president of the United States has
adopted and implemented the 15-minute coronavirus test, to the extent that no one can
come near him until they have taken the 15-minute coronavirus test. Naturally, the
president and coronavirus task force are moving heaven and earth to extend this
life-saving measure to all senior citizens.
... in this crisis, a single-buyer - single-payer system for the acquisition of critical care
medical and hospital equipment and supplies, must be implemented.
... the glaring element missing from both the Canadian and the United States
coronavirus mitigation campaign, is a rigorous contact management regime,
whereby you trace everyone and anyone who has come into contact
with a person who tests positive, and place them under quarantine.
... the 15-minute coronavirus test, when implemented properly,
will reduce the iatrogenic transmission of the coronavirus by health care workers,
caregivers & essential services workers, and all with whom they interact to a minimum.
... it should not go unnoticed, how quickly the president of the United States has
adopted and implemented the 15-minute coronavirus test, to the extent that no one can
come near him until they have taken the 15-minute coronavirus test. Naturally, the
president and coronavirus task force are moving heaven and earth to extend this
life-saving measure to all senior citizens.
... in this crisis, a single-buyer - single-payer system for the acquisition of critical care
medical and hospital equipment and supplies, must be implemented.
... the glaring element missing from both the Canadian and the United States
coronavirus mitigation campaign, is a rigorous contact management regime,
whereby you trace everyone and anyone who has come into contact
with a person who tests positive, and place them under quarantine.
By the autumn of 1918, the virus that caused the Spanish flu had not only circumvented the globe, after the first case had been reported at a military base in the State of Kansas in the early spring of 1918, but the virus had by then mutated into a vastly more potent strain, and unleashed an unremitting - second wave - of the Spanish flu pandemic that could kill even a young, healthy person, within 24 hours of the first signs of the onset of illness.
And, lest we forget that as the 2002 SARS pandemic waned in 2003, and in fact, the City of Toronto was thought to have been free of any cases of local transmission of the SARS virus for more than four weeks, a single hospital proved to be the epicenter of a second wave of that pandemic that lasted until 2004.
As is now known, patients undergoing long-term treatment for pneumonia (pneumonia used here euphemistically for a range of immune deficient patients) harboured the SARS virus. A lack of new transmissions in the community led to a relaxation of the hospital's infection and disease control measures, which exposed health care workers to the virus. As a consequence, over 40% of the SARS infections during the second wave of the Toronto outbreak were health care workers.
Today, we can compare the outbreak among health care workers in Massachusetts to those in Toronto, and as a presumptive explanation for the recent outbreak in St Albert, Alberta.
It should be noted that the 2002-2004 SARS virus never went away actually, but the number of cases in Canada was reduced to no more than 100 a year. And, it should be noted that a second strain of the current SARS-CoV-2 virus has already been isolated and identified.
We often hear analogies made to fighting a war in relation to efforts to counter the worst possible outcomes of the coronavirus pandemic, as well as, to convey a sense of urgency to these efforts.
But, let us take a closer look at the realities of fighting a war.
The first thing that can be observed when a battle, that is, the fighting actually begins, is that there are casualties on both sides. This is one of the core essential realities of war, there will be casualties on all sides.
Continuing to equate waging war to the coronavirus campaign, no commander would engage in battle with the belief that 100% of their human and material resources would be deployed with 100% efficiency, 100% of the time.
Nor, conversely, would a commander assume that 100% of the human and material resources of the opposing forces would be 100% ineffective, 100% of the time.
Let us say that a commander deployed human and material resources with sterling efficiency. At that level, 92.5% of the resources available could actually be engaged in battle, leaving 7.5% of resources idle for various reasons. Importantly, therefore, if you want to put 100 units of human and material resources into battle, you have to have 107+ units available to deploy your resources at the sterling level of efficiency.
The lesson here is that hospital equipment used in critical care and infectious disease control environments is not, cannot and will not be deployed with sterling efficiency. The schedule for the routine maintenance, re-calibration and cleaning between patient use of such equipment is one part of a rigorous campaign against cross infection waged by hospitals, continuously.
One last word of caution, it is assumed that the ventilation systems in the buildings being used as temporary hospitals, have been screened for all the known germs that dwell in ventilation systems. In hospitals, not only is the treatment delivery equipment placed under a schedule for routine cleaning and maintenance, but the entire wards themselves. And, it ought to be considered that the more intense the use of critical care and infectious disease control facilities, the shorter the interval between the application of stringent infection and disease control measures. Otherwise, these facilities would rather quickly become sick buildings, and have to be closed, decommissioned, altogether.
When one listens to or reads the safety instructions before a flight, one of the instructions concerns, what will happen, and what one should do in case of a sudden fall in cabin pressure.
The what, is that a facemask connected to an air supply will be released from above each seat location. And, what one should do in that case, if you are an able adult, is to put a mask on yourself first, and then you will be in a position to assist a child or anyone unable to place the mask on themselves. Otherwise, not only can you not help someone else, but you will become someone in need of help yourself.
Mid-week, according to ISO 8601, which began on Monday the 16th of March, the president of the American Hospital Association, during a singular cable news interview, stated that there was, albeit then of limited scope, an FDA approved 45-minute test for the coronavirus. In fact, the hospital association president stated that the test took 45 minutes to one hour to get a result that would identify whether the tested individual was positive, infected with the coronavirus, or negative, not infected with the coronavirus.
What took place over the next several days without political posturing, outside the glare of crusading and issue framing cable news programming, and continuing our war-footing analogy, without raising the ire and inciting the obstructionist activities of fifth-columnists, was a thoughtful discussion within the medical community and between the medical community and the FDA, which first recognized that any decision by the FDA had to be based preeminently on the efficacy of the test itself. And yet, again without fanfare, resulted in the FDA approval of a 45-minute coronavirus test for use in all fifty states.
Importantly, just eight days later, the FDA announced (14:00 hrs EST, 28 March 2020) its approval of a 15-minute coronavirus test, which had also been in the trial and verification process.
And through existing protocols, if they so choose, the 45-minute, and the 15-minute coronavirus tests are available to our North American partners and international agreements extend its use to others, who choose to avail themselves of these highly valuable medical screening tools.
There should be no doubt that the 15-minute coronavirus test, the ability to know whether a person is positive for coronavirus, in real time, instituted properly, will prove beneficial.
... the 15-minute coronavirus test, when implemented properly, will reduce the iatrogenic transmission of the coronavirus by health care workers, caregivers, as well as, essential services personnel to a minimum.
As an example, let us consider shift change at a fire or a police station. All personnel entering the station report 20 minutes to 1/2 hour, on the clock as it were, before the start of their duty. They drive through the mobile testing station, get swabbed, proceed to the parking lot, and are notified of the result of their test within 1/2 hour. If, the test is negative, they proceed into the station.
Those leaving the station go through the same procedure. Any personnel whose duty requires them to remain in the station, departs with those leaving the station and proceeds to the testing area for those seeking to enter, and are tested before they re-enter to resume their duty.
This testing regime requires that there is a plan in place to replace personnel that test positive. And, that there is a plan in place as to where patients that test positive are to be cared for and by whom.
In the letter to Premier Jason Kenney, below, suggesting that all patients in hospital with pneumonia, the lesson of the second wave of SARS 2002-2004, be tested for the coronavirus, becomes possible in real time with the 15-minute test.
As in the case of firefighters, all health workers are screened before entering the hospital, and if they test negative, they proceed to their hospital stations. It is this group that then screens all the patients in hospital. The staff leaving is tested and if any health care worker tests positive, if they are qualified to do so, before they leave the parking lot, they are supplied with enough kits to test all the members of their household, or anyone else they have come into contact with within their own home, in which they will now be self quarantined.
The same testing regime, as a matter of the utmost urgency, must be implemented in all nursing homes, hospice care centres and veteran's hospitals. Screen everyone entering, those cleared to enter test all residents in the facility, any workers remaining at shift change, depart the facility with other workers ending their shift and join the queue of those being tested to enter the facility, without exception.
Evidence supports the realization that those in hospital being treated for pneumonia, those in-hospital patients who are immune deficient, the elderly in nursing homes, our veterans in VA hospitals, an all those under hospice care, and those that care for them, must be tested for the coronavirus, and the 15-minute coronavirus test, implemented properly, is a reasonable means to do so.
To have the 15-minute test and not implement a procedure to protect the public as well as our essential workers, ought to be unthinkable.
This communication is being sent to the governors of the states and territories of the United States, the premiers of the provinces and territories of Canada, and the prime minister of Australia.
Communication with the global medical and scientific community is an ongoing state of affairs which stems from and reflects this author's decades-long international health care career.
There is an appendix to this document, under separate cover, addressed to the premier of Alberta, the governor of California and the prime minister of Australia, each of whom are on the cusp of yet another devastating fire season. And, each of whom shares the ominous distinction of having been the chief executive of their respective governments, when smoke from wildfires (bushfires) killed far more of their citizens than did the fires.
The premature deaths due to smoke inhalation, during the 2020 fire season, will occur at the same time as an equally devastating viral respiratory disease pandemic. The sudden and dramatic increase in the demand for ventilators and ICU facilities during previous fire seasons should spur preparation for the next one.
The Oxford Textbook of Infectious Disease Control
Let us consider how infectious disease control ought to be organized, by the textbook, as it were.
Our real-life example of the implementation of an evidence-based, epidemiologically sound infectious disease control program, which includes both surveillance and a rigorous contact management strategy, is Iceland.
We will address the, Oh, Iceland can do that because they are small, rejoiner, but suffice it to say that in reality, we all live in relatively small neighborhoods, or we can organize our neighborhoods into more manageable sized entities, limited only by our collective imaginations.
After several hundred people had tested positive for the coronavirus in hospitals in Iceland, health authorities and university researchers devised an initiative that would draw thousands of people from the general public in to be tested for the coronavirus.
Those with symptoms were asked to go to hospital for testing, and those without symptoms who wished to be tested, could do so, free of cost, at a number of locations. Those who were symptom free and in self-quarantine could be tested in situ.
As a result of the in-hospital and community-based coronavirus surveillance initiative, 1200 individuals were identified to be positive for infection with the coronavirus. And, by the first day of April, two people had died from complications arising from their infection with the virus.
The in-hospital testing of those with flu-like symptoms identified 600 cases of infection with the coronavirus. The community-based surveillance initiative of those showing no symptoms uncovered another 600 individuals who tested positive for the virus.
Textbook infectious disease control principles and procedures dictate that health departments and the responsible officials within them, identify and locate every individual who has been in contact with every individual who tests positive for an infectious disease, and place them under quarantine, without exception and without delay. The process of doing so is known as rigorous contact management.
The Icelandic infectious disease control personnel interviewed every individual both in-hospital and in the community who tested positive, and produced a list of all persons, whose contact with an infected person fit the criteria of the interaction with a person who tested positive could be described as close contact.
In total, the infectious disease control team collected the names of 7800 individuals identified as having had close contact with one of the individuals who tested positive for the coronavirus. Therefore, each infected individual had had close contact with 6.5 other persons, on average. Who, from a infectious disease control perspective fit the criteria for being placed under quarantine.
More than 7,800 others were in quarantine, and more than half of those who had been diagnosed with the virus were already in quarantine at the time of their diagnosis, according to official government data.
During an infectious disease control emergency, contact with an infected person is sufficient cause for placing an individual under quarantine.
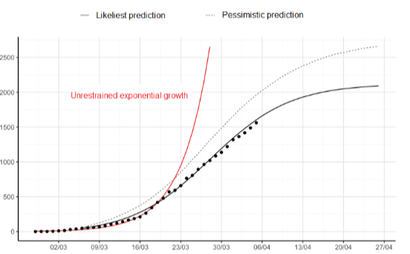
Observe the graph below, which depicts the profound results that can be achieved
Our real-life example of the implementation of an evidence-based, epidemiologically sound infectious disease control program, which includes both surveillance and a rigorous contact management strategy, is Iceland.
We will address the, Oh, Iceland can do that because they are small, rejoiner, but suffice it to say that in reality, we all live in relatively small neighborhoods, or we can organize our neighborhoods into more manageable sized entities, limited only by our collective imaginations.
After several hundred people had tested positive for the coronavirus in hospitals in Iceland, health authorities and university researchers devised an initiative that would draw thousands of people from the general public in to be tested for the coronavirus.
Those with symptoms were asked to go to hospital for testing, and those without symptoms who wished to be tested, could do so, free of cost, at a number of locations. Those who were symptom free and in self-quarantine could be tested in situ.
As a result of the in-hospital and community-based coronavirus surveillance initiative, 1200 individuals were identified to be positive for infection with the coronavirus. And, by the first day of April, two people had died from complications arising from their infection with the virus.
The in-hospital testing of those with flu-like symptoms identified 600 cases of infection with the coronavirus. The community-based surveillance initiative of those showing no symptoms uncovered another 600 individuals who tested positive for the virus.
Textbook infectious disease control principles and procedures dictate that health departments and the responsible officials within them, identify and locate every individual who has been in contact with every individual who tests positive for an infectious disease, and place them under quarantine, without exception and without delay. The process of doing so is known as rigorous contact management.
The Icelandic infectious disease control personnel interviewed every individual both in-hospital and in the community who tested positive, and produced a list of all persons, whose contact with an infected person fit the criteria of the interaction with a person who tested positive could be described as close contact.
In total, the infectious disease control team collected the names of 7800 individuals identified as having had close contact with one of the individuals who tested positive for the coronavirus. Therefore, each infected individual had had close contact with 6.5 other persons, on average. Who, from a infectious disease control perspective fit the criteria for being placed under quarantine.
More than 7,800 others were in quarantine, and more than half of those who had been diagnosed with the virus were already in quarantine at the time of their diagnosis, according to official government data.
During an infectious disease control emergency, contact with an infected person is sufficient cause for placing an individual under quarantine.
Observe the graph below, which depicts the profound results that can be achieved
Click on the link, below, to read the full report of the Covid-19 mitigation campaign in Iceland, conducted by the
University of Iceland’s Health Sciences Institute, the Directorate of Health, and the National Hospital of Iceland -
https://covid.hi.is/english/
_ _ _ _ _ _
University of Iceland’s Health Sciences Institute, the Directorate of Health, and the National Hospital of Iceland -
https://covid.hi.is/english/
_ _ _ _ _ _
New Rochelle is Governor Cuomo's Waterloo
... operation market garden
Governor Andrew M Cuomo is not the first chief executive or commander to order forces into the field, and then hesitate inexplicably, and not deploy them efficiently or effectively to the task at hand, far from it.
In a seminal contribution to military history 'The Ardennes on Fire', Timothy J Thompson chronicles how the allies with superior forces, an opportunity to finish off the Third Reich, allowed the Germans to re-establish and actually gain the upperhand. This cost the lives of thousands of allied forces. Thompson writes:
"Although Germany had made a miraculous recovery in terms of manpower on the Western Front during September 1944, they were still in dire straits. The newly acquired forces had not been properly trained; even in the most rudimentary sense of sound infantry tactics. In addition, they were still woefully short of [small] arms, like heavy machine guns, long range artillery, and heavy tanks. Those would not arrive in force until late October. The Allies still had an opportunity to finish off the Third Reich, once and for all, before Christmas.
On September 10, a plan was hatched to do just that. It was called: Operation Market Garden. It was the brain child of British Field Marshal Sir Bernard Law Montgomery. He was in command of the British 21st Army Group. This consisted of the British Second Army under General Dempsey, and the Canadian First Army under General Crerar. Together, they amassed just under 200,000 men.
Montgomery was an extremely overly cautious commander. Repeatedly, he would delay action until he possessed overwhelming supremacy in every appreciable category imaginable. In this sense, he was not unlike the Union General George B. McClellan during the American Civil War [1861-1865]. In spite of this, he would often times execute the subsequent attack with Neolithic incompetence wrought on by the utter inability to properly handle massed armored formations in the open."
When Governor Cuomo ordered National Guard troops into New Rochelle, a sense of quiet optimism circumvented the globe, from London to Reykjavik, in Milan where health authorities were bewildered by the contrast between an unfolding health crisis and a lethargic response by the national government, it seemed that albeit not coming from Washington, the Americans had awaken to the rather stark reality of a pandemic.
Why would Governor Cuomo order troops into New Rochelle, those observing his actions from near and far wondered ?
What was desperately needed at that precise juncture was to assist, if not to initiate, in conjunction with local area health departments, a by-the-book, first-phase infectious disease control management plan, which calls for the identification of cases of infected persons, and then to contact anyone and everyone who has come into contact with an infected individual and quarantine them, immediately.
All other measures of infectious disease control and mitigation, including hygiene, social distancing, and even vaccinations are designed to augment the most basic means of infectious disease control i.e., case identification and contact tracing, but not to replace case identification and contact tracing.
When Governor Cuomo failed to engage the troops he ordered into New Rochelle into the basic actions of infectious disease control, he assured that the trajectory of cases in New York would resemble the red line in the graph above, entitled 'Unrestrained exponential growth', as opposed to the solid line with the superimposed dots, which resulted from identifying 1200 cases and contact tracing 7800 individuals, who had had contact with the identified cases and placing them in quarantine.
There is no middle ground.
Naturally, the entourage of people surrounding, now protecting Governor Cuomo from information coming into his administration from the outside, including, if not especially his health officials, could and would not countenance the suggestion that the Governor's response, or better the lack of a coherent response by the health officials of his government, jointly and severally, constitutes malfeasance, bordering on criminal negligence, go without comment.
The retort suggests; Okay, the troops trace everyone of the contacts of the first 50 people known to have been exposed in New Rochelle, which in the immediate aftermath was some 300 people. And, with the delay in initiating a rigorous contact tracing of those 300, the number had grown to 1800 possible infections with the virus. But, they suggest, we get the name of a person and that person is in Phoenix, Chicago or Seattle the next day, so what have we accomplished?
If there ever was a sterling example of the proof that ignorance is bliss, this should make the hall of shame.
What have we accomplished?
In reality, there are 2,800 local health departments across the United States, these comprise city, county, metropolitan, district and tribal departments. In addition, there are 126 health regions in Canada. Therefore, a person leaving New Rochelle and travelling to Phoenix, Chicago, Seattle, Vancouver or Toronto, is moving from one health district into another one.
The more pertinent question is what are the consequences of not having implemented an immediate regime of case identification and rigorous contact tracing?
The most obvious answer is the existence of mass graves in 21st century New York.
Governor Cuomo, has of late, thought it appropriate to quote the likes of FDR and Winston Churchill, however, this author proposes a military doctrine that is related directly to the task at hand, the Gregory Doctrine, which states:
A deterrent is always better than a response.
That brief optimism felt around the world, when Governor Cuomo ordered the troops into New Rochelle, was that finally a leader in one of the major liberal democracies was going to deploy the resources, and those resources are layers deep, at hand to do the straightforward task of case identification and contact tracing. And, thereby slow the spread of the coronavirus to levels seen in Iceland, Taiwan & Shanghai.
But that did not happen, the troops became no more than glorified traffic watchers.
It is not too late for many other communities, since this author has been trying to get through to Mayor Lightfoot of Chicago, for example, the numbers in the entire state of Illinois have grown from less than the 1200 cases the authorities in Iceland had to confront, and a fraction of the contacts to be traced in Shanghai, to now well over 75,000.
Which begs the question, what have the 2,926 heads of the health departments and heath regions in the United States and Canada, those highly paid health officials responsible for infectious disease control, been doing since the outbreak of the coronavirus?

Click on banner above, or link below, to read part 4 of this series on the coronavirus.
https://www.theoxfordscientist.com/coronavirus-a-perfect-storm.html
https://www.theoxfordscientist.com/coronavirus-a-perfect-storm.html
_ _ _ _ _ _
This copy of the original letter to Premier Jason Kenney of Alberta, I submit to your thoughtful consideration.
The letter was updated to include a caution issued by the World Health Organization (WHO) concerning the use of ibuprofen
and other NSAIDs by those self-medicating who may be coronavirus positive.
The letter is also historic. It was written at a time when the State of New York, including New York City, had tested some 10,000 individuals,
2382 of whom tested positive for the coronavirus and, 594 of those who tested positive required hospitalization.
The letter suggests that there are three things that must be implemented in short order,
the 15-minute coronavirus test, should help us accomplish two of them.
_ _ _ _ _ _
This copy of the original letter to Premier Jason Kenney of Alberta, I submit to your thoughtful consideration.
The letter was updated to include a caution issued by the World Health Organization (WHO) concerning the use of ibuprofen
and other NSAIDs by those self-medicating who may be coronavirus positive.
The letter is also historic. It was written at a time when the State of New York, including New York City, had tested some 10,000 individuals,
2382 of whom tested positive for the coronavirus and, 594 of those who tested positive required hospitalization.
The letter suggests that there are three things that must be implemented in short order,
the 15-minute coronavirus test, should help us accomplish two of them.
_ _ _ _ _ _
The Honourable Jason Kenney
Premier of Alberta
Sir,
If, one wants to understand the cluster of coronavirus cases in the Red Deer area or more recently in St Albert, it is explained by the most fundamental understanding of the spread of disease known to medical science, that is, disease follows migration, independent of the mode or the means of transportation.
More than 10,000 individuals have been tested in a score of counties in the State of New York, 2382 of those tested proved positive for the coronavirus. 549 of those who tested positive (23%) required hospitalization. Of those hospitalized, an alarmingly high number were under fifty (50) and otherwise healthy.
There are three things, you as the chief executive of this province, will have to implement in rather short order.
One, all patients in hospital with pneumonia of unknown cause, must be tested for the coronavirus.
Two, because all patients with pneumonia of unknown cause have not been tested for the coronavirus, it is critical that all healthcare workers be tested for the coronavirus.
Three, anecdotal evidence has existed since the SARS pandemic that the drug ibuprofen increases the severity of some viral respiratory diseases. There are otherwise healthy young people in hospitals in Canada, Europe and the USA, who are on ventilators, with the common denominator of having tested positive for the coronavirus and having ingested ibuprofen.
Increasingly, health authorities are now taking aspirin, acetaminophen (paracetamol), ibuprofen and a host of other pain treatments out of the over-the-counter system, and placing them with pharmacists, who can ascertain the reason a person is seeking pain relief and steer those who might be coronavirus positive away from ibuprofen.
As long as, we are advising people to self-quarantine, and they continue to self-medicate, removing ibuprofen from the shelves is the prudent course of action.
Kindly note, since this information was published, the airways have been full of contradictory statements on this issue. European health authorities continue to remove ibuprofen from the over-the-counter system, the French and Italian experience is noteworthy. We know how to conduct a clinical trial to bring the anecdotal onto a firm scientific basis.
In the interim, the precautionary principle must guide clinical practice and health care advice.
In keeping with the fundamental principle of doing no harm, on Tuesday, the World Health Organization, WHO, recommended that ibuprofen and other NSAIDs drugs should not be taken. The most recent concerns about ibuprofen arose as a result of a study published in the medical journal The Lancet, and voiced by French Health Minister, Olivier Veran.
The issue of self-medicating in the midst of a pandemic must be addressed, and sound health advice is wanting.
I anticipate sound advice from your administration, Premier Jason Kenney.
I remain at your disposal.
Best regards,
E LaMont Gregory MSc Oxon
- - - - - -
Premier of Alberta
Sir,
If, one wants to understand the cluster of coronavirus cases in the Red Deer area or more recently in St Albert, it is explained by the most fundamental understanding of the spread of disease known to medical science, that is, disease follows migration, independent of the mode or the means of transportation.
More than 10,000 individuals have been tested in a score of counties in the State of New York, 2382 of those tested proved positive for the coronavirus. 549 of those who tested positive (23%) required hospitalization. Of those hospitalized, an alarmingly high number were under fifty (50) and otherwise healthy.
There are three things, you as the chief executive of this province, will have to implement in rather short order.
One, all patients in hospital with pneumonia of unknown cause, must be tested for the coronavirus.
Two, because all patients with pneumonia of unknown cause have not been tested for the coronavirus, it is critical that all healthcare workers be tested for the coronavirus.
Three, anecdotal evidence has existed since the SARS pandemic that the drug ibuprofen increases the severity of some viral respiratory diseases. There are otherwise healthy young people in hospitals in Canada, Europe and the USA, who are on ventilators, with the common denominator of having tested positive for the coronavirus and having ingested ibuprofen.
Increasingly, health authorities are now taking aspirin, acetaminophen (paracetamol), ibuprofen and a host of other pain treatments out of the over-the-counter system, and placing them with pharmacists, who can ascertain the reason a person is seeking pain relief and steer those who might be coronavirus positive away from ibuprofen.
As long as, we are advising people to self-quarantine, and they continue to self-medicate, removing ibuprofen from the shelves is the prudent course of action.
Kindly note, since this information was published, the airways have been full of contradictory statements on this issue. European health authorities continue to remove ibuprofen from the over-the-counter system, the French and Italian experience is noteworthy. We know how to conduct a clinical trial to bring the anecdotal onto a firm scientific basis.
In the interim, the precautionary principle must guide clinical practice and health care advice.
In keeping with the fundamental principle of doing no harm, on Tuesday, the World Health Organization, WHO, recommended that ibuprofen and other NSAIDs drugs should not be taken. The most recent concerns about ibuprofen arose as a result of a study published in the medical journal The Lancet, and voiced by French Health Minister, Olivier Veran.
The issue of self-medicating in the midst of a pandemic must be addressed, and sound health advice is wanting.
I anticipate sound advice from your administration, Premier Jason Kenney.
I remain at your disposal.
Best regards,
E LaMont Gregory MSc Oxon
- - - - - -
Trump's folly
advertisement circa 1918
advertisement circa 1918

